Arterial Line Basics for Critical Care Nurses
Arterial line management is one of the most foundational skills that critical care nurses need to have. The understanding of arterial lines goes much deeper than simply seeing the numerical value that is represented on your bedside monitor. Proper management includes:
- Proper Setup
- Calibration of the System
- Waveform Analysis
- Troubleshooting
Don’t forget to grab your free Arterial Line Management Resource Here.
Before we can move forward with diving deep into Arterial Lines, let’s discuss why we use – and love – them in Critical Care areas.
Why we use Arterial Lines in Critically Ill Patients:
There are two main reasons why we arterial lines get placed on our patients:
- Continuous Hemodynamic Monitoring – The biggest benefit of an arterial line is that it provides us with real time beat-to-beat readings on our patients blood pressure. This is incredibly helpful if we are managing a patient who is on continuous vasoactive medications. Rather than waiting for a non-invasive blood pressure to cycle, which isn’t accurate in critically ill patients, we can see changes in our patients’ blood pressure as soon as they occur. However, that isn’t the only way that arterial lines provide us with information regarding our patients’ hemodynamics. There are some technologies that use arterial line waveform analysis to give additional data around cardiac output, stroke volume, stroke volume variance, ect.. I talked about that in my Ultimate Hemodynamic Resource.
- Ease of Arterial Blood Sampling – At times our patients will require multiple arterial blood samplings, and having an arterial line makes it easier for not only the patient but for us as well. Rather than the patient having to be stuck multiple times, they can have a small catheter placed in the artery that then allows for us to obtain samples when needed. This can be especially helpful if our patients are on high ventilatory support.
Providers will ultimately make the decision on if the patient needs to have an arterial catheter placed or not. Once that decision is made, as critical care nurses we typically will be assisting with the process by setting up the monitoring system.
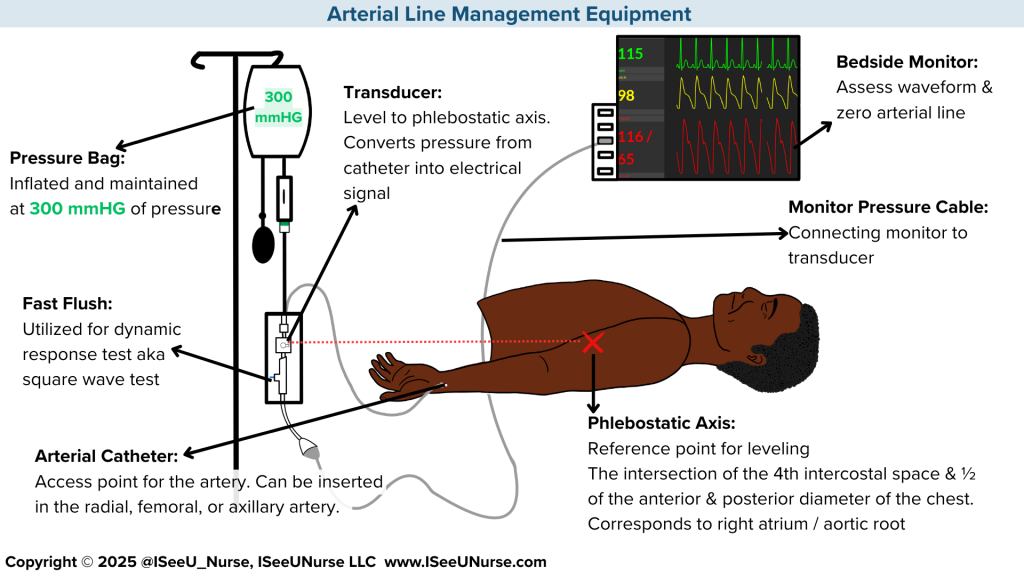
The setup of a hemodynamic system can influence the accuracy of the readings obtained on the monitor. Below is an image of all of the major pieces needed to properly setup an arterial line.
As far as the actual set up, here are some of the top errors that will contribute to inaccurate readings:
- Check your connections. When you get the system out of the package, the first thing to do is make sure all the connections are tightly secured. They may seem like they are visually secure, but double check. Often times they are a little loose and you don’t want an accidently disconnection at some point when it is connected to a patient.
- Don’t add extension tubing, if you can. Sure, there will be some very specific moments when extension tubing may be needed. However, in general try to avoid adding anything additional to the standard system. Extension tubing can contribute to an improperly dampened waveform. Also, if you are going to add extension tubing – it needs to be the same rigid tubing that comes with the system. It cannot be regular extension tubing.
- Ensure All Air is out of the Priming Solution. Correctly priming the system involves removing all of the air out of the (typically) NaCl bag. This involves spiking the bag, keeping the bag and spike upside down, and pulling the fast flush to remove all of the air. This important step ensures there is no risk of an air embolism to your patient. Unlike IV pumps, there isn’t an alarm that will alert you if there is air in the system.
- Don’t prime under pressure. Initially the system needs to be primed without pressure, and once the priming solution is to the end of the tubing, then it can be inflated. This prevents micro air bubbles which can cause inaccurate readings, specifically it can contribute to an overestimation of systolic blood pressures and an underestimation of diastolic blood pressures.
- Ensure proper inflation. After the system is properly primed, the pressure bag must be inflated to the proper amount of 300 mm HG. This allows for patency of the catheter itself and ensures that there isn’t going to be a backflow of blood from the artery when connected.
- Replace the vented cap. When you initially grab the arterial line set up out of the package, there is a vented cap on the all stopcocks. As in, the opaque cap on the stopcock has a hole in it. Best practice is to change that vented cap to one that is non-vented. Typically systems will have a non-vented cap in the packaging. The rationale behind changing to a non-vented cap is that it reduces the risk of infection, air entering into the system, and lowers the risk of backflow of blood if the stopcock arrow accidentally was in the improper position.
As you can see, there are many nuances involved with the set up of the system in order to avoid any erroneous readings on the bedside monitor. However, set up isn’t the only thing we must pay attention to. The next step: calibration of the system is equally as important. We will cover that in the next post.